Double Vision After Eye Injury
How specialists evaluate diplopia after trauma and what treatment pathways exist.
Double vision (diplopia) after trauma can be frightening, but it isn’t one diagnosis—it’s a symptom. The cause can be temporary swelling, a fracture, nerve-related changes, or a shift in the eye’s position inside the orbit.
The goal of evaluation is to identify whether diplopia is expected to improve on its own—or whether it suggests a structural issue that benefits from imaging and targeted treatment.
For a full list of trauma-related concerns we evaluate, visit Eye Trauma.
At a Glance
- Common cause: swelling affecting movement
- Structural cause: fracture/entrapment
- Exam: alignment + motility testing
- Urgent signs: severe pain, vision loss, inability to move eye
- Imaging: CT often used if fracture suspected
- Goal: comfortable single vision
Why diplopia happens after trauma
- Swelling/bruising that temporarily limits muscle function
- Orbital fracture with tissue or muscle restriction
- Nerve-related changes affecting muscle control
- Eye position changes altering alignment
- Less commonly, issues affecting the clarity of vision in one eye
The timing of diplopia, what directions trigger it, and whether movement is restricted are all diagnostic clues.
Red flags to treat as urgent
Seek urgent in-person care for sudden vision changes, severe escalating pain, inability to move the eye in certain directions, significant nausea/vomiting with attempted eye movement, or rapidly worsening swelling.
Persistent diplopia that interferes with walking, driving, or reading deserves timely evaluation.
A realistic healing timeline (what you might notice)
Healing varies, but many patients describe a similar pattern:
- Days 1–3: swelling and bruising can peak; it may look worse before it looks better.
- Days 4–7: swelling begins to soften; comfort often improves; early contour becomes easier to assess.
- Weeks 2–4: bruising fades; symmetry and function become more stable; ongoing irritation should be improving.
- Months 2–6: scars and subtle contour changes continue to refine; final “settled” appearance becomes clearer.
What matters most is the trend. Steady improvement is reassuring. New or worsening functional symptoms deserve a check‑in.
Common myths (and what’s actually true)
- Myth: “If it doesn’t hurt much, it can’t be serious.”
Reality: Some injuries affect alignment, drainage, or eyelid position with surprisingly little pain. - Myth: “If the skin is closed, everything underneath is fine.”
Reality: Inner-corner injuries can involve tear drainage, and fractures can change eye position even after swelling resolves. - Myth: “I should just wait until swelling is completely gone.”
Reality: Early evaluation can be important for time‑sensitive issues and creates a baseline for safe observation.
The goal isn’t to overreact—it’s to match your symptoms to the anatomy that was injured, so you don’t miss a fixable problem.
What the exam evaluates
A structured evaluation often includes vision and pupil assessment, motility testing in multiple directions, alignment checks in primary and reading gaze, eyelid position assessment, and review of imaging when fracture is suspected.
This helps differentiate swelling-related limitation from mechanical restriction or displacement.
Treatment pathways
Depending on findings, your plan may include:
- Observation with follow-up measurements (if improvement is expected)
- Orbital fracture repair when restriction/displacement is significant
- Temporary prism correction for select cases during healing
- Additional specialty evaluation if alignment issues persist
A good plan focuses on function: achieving comfortable single vision in the gaze positions you use most.
Recovery and follow-up milestones
Many patients notice improvement as swelling resolves over days to weeks. Follow-up visits track whether alignment is improving at the expected pace.
If symptoms plateau or remain disruptive, your care team can reassess imaging and discuss next steps rather than continuing to wait without direction.
What to watch for during the first two weeks
The early healing period is when you’ll notice whether symptoms are trending in the right direction. It’s helpful to track:
- Whether swelling is steadily improving
- Whether comfort is improving with blinking and screen time
- Whether tearing or dryness is changing
- Whether eyelid contour looks more stable day to day
If something is getting worse instead of better, that’s a reason to contact your surgeon.
A simple next‑steps plan
If you’ve had an eyelid or orbital injury and you’re unsure what matters most, a structured evaluation is the fastest way to clarity. You can review what’s treated and what to expect on our Eye Trauma page, then schedule an appointment for individualized guidance.
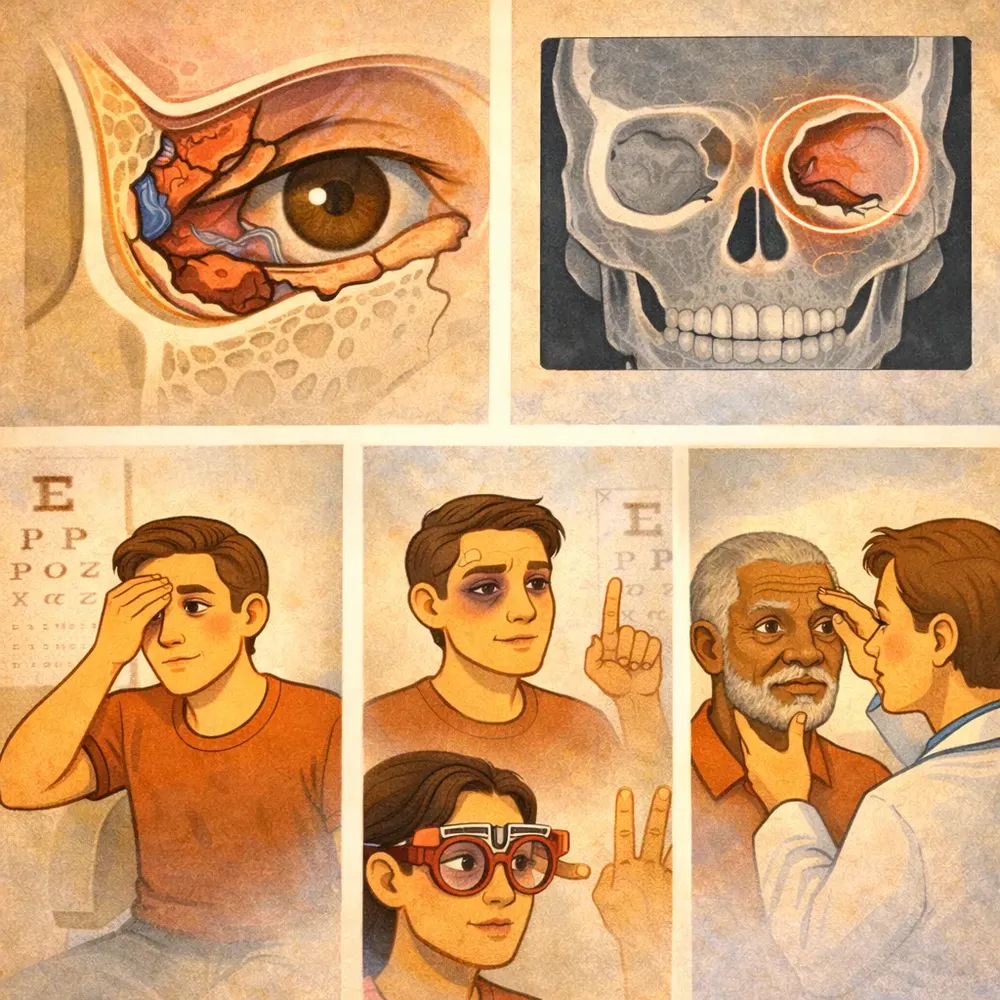
A clear explanation of “entrapment”
Entrapment occurs when soft tissue is restricted by the fracture site. It can create a distinct pattern of movement limitation and diplopia. Not all fractures cause entrapment—so imaging and exam findings need to match.
That’s why a specialist doesn’t treat the scan alone; they treat the scan plus the symptom pattern.
What to track before your visit
- Which direction triggers diplopia the most
- Whether it’s worse in the morning or later in the day
- Whether you have associated pain with movement
- Whether the eye looks positioned differently than before
Specific details help correlate symptoms with anatomy.
Frequently Asked Questions
How long does double vision last after an injury?
It varies. Some cases resolve as swelling improves; others require imaging and targeted treatment. Persistent diplopia should be assessed.
Can diplopia be caused by swelling only?
Yes. Swelling can temporarily limit movement. The exam helps determine whether observation is safe.
Should I wait weeks before seeing a specialist?
If diplopia is significant, persistent, or associated with restricted movement, earlier evaluation is better.
What should I do if symptoms change suddenly?
Sudden vision changes, severe pain, or rapidly worsening swelling should be evaluated urgently in person.
What should I do if symptoms change suddenly?
Sudden vision changes, severe pain, or rapidly worsening swelling should be evaluated urgently in person.
How can I tell if things are improving normally?
Normal recovery usually shows gradual improvement in comfort, swelling, and function over time. If you notice worsening pain, new vision changes, or a new functional limitation, seek in‑person evaluation.
Why See an Oculoplastic Surgeon?
Trauma care often needs a balance of function (vision, comfort, eyelid closure, tear drainage) and appearance (symmetry, natural contour). An oculoplastic surgeon is specifically trained for eyelid, tear duct, and orbital reconstruction.
Alexander Rabinovich, MD provides oculoplastic trauma evaluation and reconstruction in New York City and Brooklyn. Because diplopia can come from orbital anatomy, eyelid position, and fracture effects, a trauma-focused oculoplastic evaluation can be especially helpful.
Educational content only; not a substitute for medical advice. If you have sudden vision changes, severe pain, or worsening symptoms after an injury, seek urgent in-person care.
Book a Double Vision Evaluation
For an overview of services and what we treat, visit Eye Trauma. You can also book a consultation below.

Leave a reply